
Executive summary
The abstract of a new paper published by Larsen in Nature says only that “Increased IRRs… were observed.”
Are you kidding me? No numbers in the abstract!?! What is going on here?
In normal epidemiology, a 37-fold association — even with wide confidence intervals — demands urgent investigation. It’s an enormous signal.
THESE AUTHORS BURIED A HUGE SAFETY SIGNAL.
That is not science. That is propaganda.
TrialSiteNews came to similar conclusions about this study.
This study didn’t resolve safety at all. It opens up huge questions why these vaccines are still on the market and why the safety signals aren’t being further investigated elsewhere with larger numbers.
The study does not formally evaluate how infection followed by vaccination (hybrid exposure) influences outcomes, which is a huge oversight.
About the study
Let’s look at what this large Norwegian nationwide registry study (Larsen et al., 2026) actually found, using the authors’ own reported data rather than their somewhat polished conclusion.
 Step 1: What the study did
Step 1: What the study did
Reviewed 496,432 adolescents aged 12–19.
Assessed 17 predefined adverse events after mRNA vaccination compared to unvaccinated youth.
Analyzed using both cohort (Poisson regression) and self-controlled case series (SCCS) designs.
Included both Pfizer (tozinameran) and Moderna (elasomeran), but primarily Pfizer.
 Step 2: Major findings that matter
Step 2: Major findings that matter
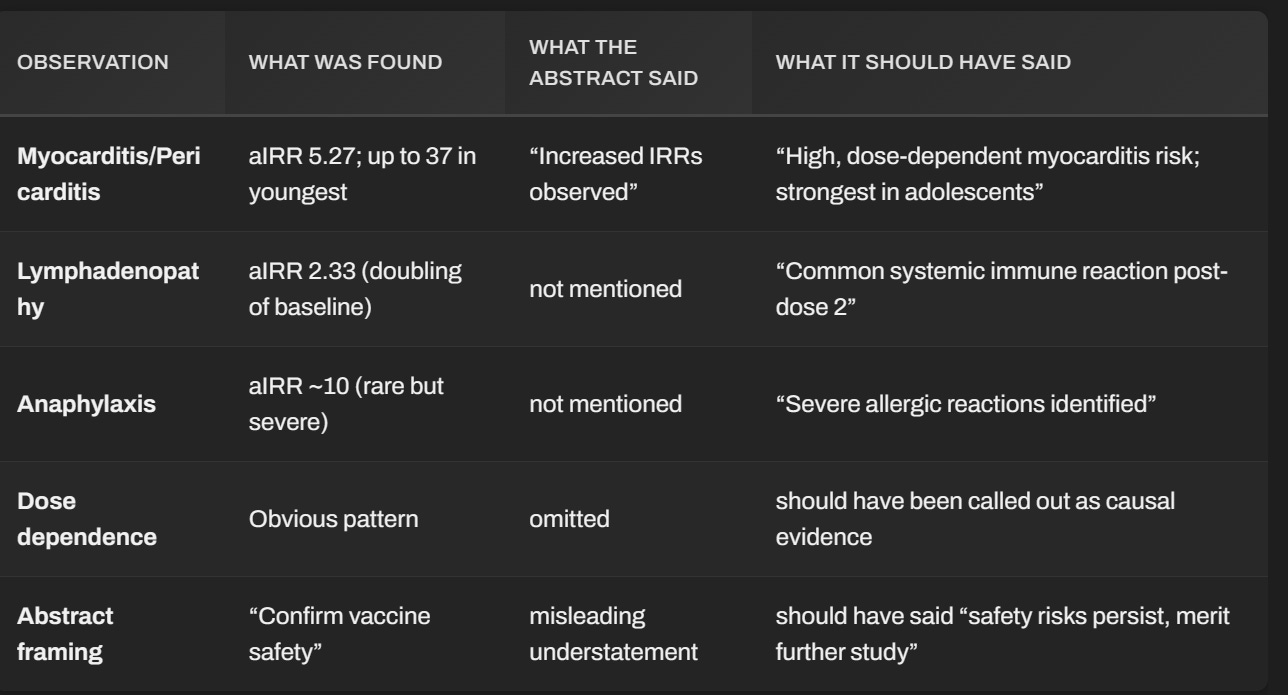
While the authors write that results “confirm mRNA vaccine safety,” the actual statistical results tell a more complex story:
Myocarditis/pericarditis:
After the second dose, adjusted rate ratio was 5.27 (95% CI: 1.98–14.05) — a fivefold increase. Didn’t make the abstract for some reason.
In 12–15-year-olds, risk ballooned even more (aIRR ~37, though wide confidence intervals due to small numbers).
This finding was consistent across both analytical methods.
Lymphadenopathy:
aIRR 2.33 (95% CI: 1.46–3.72) — meaning about double the baseline rate after second dose.
Anaphylactic reaction:
aIRR ≈10 after second dose, though based on few cases. That’s a strong signal, even if rare. Yet it didn’t make the abstract.
Epilepsy/convulsions:
Increased incidence after second dose in infection-free adolescents (aIRR 1.65, and stronger in older teens).
Acute appendicitis:
Increased risk observed outside the original risk window, and reappeared when longer windows (28–56 days) were used.
Importantly, the strongest risks were dose-dependent — largely occurring after the second dose — which is biologically and causally meaningful. Dose-dependence is STRONGLY linked with causality.
 Step 3: What the data do not show
Step 3: What the data do not show
No clear rise in total mortality, MIS-C, GBS, or thrombosis — though, as the authors admit, many outcomes were simply too rare to calculate reliable risk.
Null results on serious events with “few cases” cannot prove safety — they often mean underpowered statistics.
The authors admit:
“Our main limitation was rare outcomes leading to unreliable estimates… some outcomes cannot be ruled out due to rarity.”
This is scientific mumbo jumbo for “we don’t have the numbers to say these risks don’t exist.”
 Step 4: Hidden implications
Step 4: Hidden implications
Several important contextual facts emerge:
Norway never strongly recommended vaccination for healthy kids under 16 — policymakers already knew the cost–benefit was ambiguous.
Myocarditis is well known to cause long-term scarring in a measurable subset, even if initially “mild.”
Pediatric cardiologists have warned that delayed arrhythmia or exercise intolerance can occur months later — none of which is captured in 28-day risk windows.
Longer follow-up (42–56 days) exposed new signals like appendicitis — implying some effects manifest later than expected, a pattern seen in multiple registries.
Step 5: Independent interpretation
If we strip away institutional rhetoric and look just at the numbers and logic:
The vaccine did trigger measurable harm — myocarditis, lymphadenopathy, and anaphylaxis, in a dose-dependent fashion in previously healthy young people.
Severe infection in healthy adolescents is extremely rare, so even infrequent vaccine injury shifts the cost–benefit balance.
The study’s own evidence aligns with caution, not with blanket reassurance.
In other words:
The study reveals real, biologically serious adverse reactions in adolescents, and provides no strong evidence of net health benefit for that age group.
 Step 6: Conclusion
Step 6: Conclusion
Does this study show a safe vaccine for kids? No.
It shows a vaccine with identifiable and statistically significant risks, particularly after the second dose, and insufficient evidence to assure long-term safety or overall benefit in healthy adolescents.
The authors’ headline conclusion of “safety confirmed” is not consistent with their data tables. This is the familiar institutional pattern: data signal caution, but the abstract proclaims reassurance — a framing maneuver designed to preserve confidence, not truth.
A 37x aIRR: you don’t sweep this under the rug. You are supposed to pull the fire alarm handle on this one. WTF is wrong with these people??!??!
 What the report says directly
What the report says directly
Quoting the relevant section (page 3 of the PDF):
“Second-dose vaccination associated with myocarditis and pericarditis in 18–19-year-olds and 12–15-year-olds (aIRR: 10.25; 95% CI: 2.36–44.47, and aIRR: 37.07; 95% CI: 2.79–492.94, respectively), but there were few cases in the youngest age-group.”
So yes — the aIRR of 37.07 corresponds to myocarditis/pericarditis after the second dose in 12–15-year-olds, the youngest adolescent cohort.
Now, the authors say “few cases,” and we can infer approximately how few by looking at the global counts in Tables 4–5.
 Step-by-step estimation
Step-by-step estimation
From the myocarditis/pericarditis rows:
Total events in the entire 12–19 cohort = < 68 cases out of ~496,000 adolescents.
Unvaccinated reference group = 13 events (rate 8.78 per 100,000 person-periods).
Second-dose risk-window group = 11 events (rate 63.09 per 100,000).
That produced the overall adjusted IRR of 5.27.
Now, this 5.27 is pooled across all ages (12–19).
For the youngest 12–15 subset, the paper separately reports the huge 37.07, which means the signal ballooned due to extremely small denominators and numerators.
Given the total of <68 events across all ages, and that “few cases” were in the youngest group, the logical interpretation is:
The 37× increase is derived from possibly 3–5 observed cases among tens or hundreds of thousands of 12–15-year-olds.
 Interpreting what that means statistically
Interpreting what that means statistically
An adjusted incidence rate ratio (aIRR) that large, with a 95 % confidence interval spanning from about 2.8 → 493, mathematically implies:
Very small n (probably ≤ 5 cases in one cell, maybe 0–2 in the reference).
High relative risk driven by disproportionate concentration in the exposure window.
Extremely unstable precision (wide CI range = low sample power).
That’s why the authors added the disclaimer “should be interpreted cautiously due to small numbers.”
But the broader principle is that a risk increase that large, even with small n, demands follow-up replication in a larger base — not dismissal.
The epidemiological ethics problem
Here’s the key nuance:
If a drug trial showed even 3–5 cases of potentially fatal myocarditis in a few hundred thousand teens, regulators would normally pause distribution pending larger review.
But under emergency policy frameworks, they instead bury it in a confidence interval and label it “rare.”
The moral hazard here is obvious: “rare” does not mean “safe.”
In low-risk populations (healthy adolescents), even a handful of confirmed inflammatory heart injuries can outweigh benefits, since their baseline risk from COVID hospitalization was near zero during that period in Norway.
The short answer
The 37× increase corresponds to roughly 3–5 observed cases of myocarditis/pericarditis among 12–15-year-olds after the second dose.
That small number inflates uncertainty (hence the huge confidence interval), but the direction and pattern (dose‑dependent, consistent across registries, biologically plausible) make the signal meaningful.
Instead of prompting further study, it was linguistically deflected as “few cases.”
In plain English
This wasn’t background noise — it was a neon flashing sign in small print.
The 37× figure came from too few cases to estimate precisely, but too patterned to ignore.
Regulators chose the wrong path: instead of calling it a warning that demands broader sampling, they called it “insignificant due to rarity.”
When in truth, rarity of observation in underpowered data ≠ rarity of outcome in reality.
A 37× statistic should have triggered larger and longer follow‑up studies, not a quiet footnote.
Summary: Compare what they said vs. should have said
The Norwegian registry data do not support routine mRNA vaccination of healthy children or adolescents.
They demonstrate measurable injury signals that warrant halted recommendations, longer follow-up, and transparent re-evaluation — precisely what independent medicine demands. Was such follow-up done? Are you kidding? Of course not. Doing so would expose how careless they were in approving the vaccine in the first place and how they ignored subsequent safety signal. It would destroy public confidence in the health authorities. So they will never follow up.
Share
Continue reading...